

.............................................................................................................................................................
Your Questions Answered and What We Know Today
Who uses it, how it may help and what the science says
by
Sari Harrar, AARP
Medical marijuana has been legalized in 33
states, and many medical experts now approve of its use for particular
conditions that affect Americans over the age of 50.
This year, the AARP Board of Directors
considered the emerging evidence suggesting that marijuana is helpful in
treating such conditions and symptoms, then approved a policy supporting the
use of medical marijuana in the states that have legalized it, and supporting
further research on medical use of cannabinoids to help alleviate the symptoms
of diseases and the side effects of the treatment for diseases.
Here are seven basic facts you need to know:
The Basics
1. You are on your own
You may be thinking, Hey, if it’s
"medical,” a doctor will help me navigate the green new world. Often,
that’s not so.
A few users have a medical marijuana doctor
who walks them through products and shows them how to use a vape pen. But
that’s unusual.
“Older people think
there will be a prescription waiting for them at the dispensary, like at a
drugstore,”
says Rick McKnight, 72, a retired sales executive from Ocala, Florida, who
self-treats hip pain with marijuana.
“It’s not like that.
You get your medical marijuana card. The doctor gives you some recommendations
— not a prescription. Then you’re on your own.”
2. Dispensaries
carry a dizzying variety of products
It’s like a trip to an adults-only candy
store, loaded with tinctures and oils, vape pens and “flower” (dried
marijuana), mouth sprays and skin patches, fancy chocolate truffles,
cinnamon-scented cookies, and sodas, balms and lotions, all laced with the
active ingredients in cannabis.
You’ll also find high-strength concentrates,
waxes and resins. What’s on sale differs by state, and free samples and
in-store use are against the law.
3. Today’s cannabis is super-potent
“This is not the marijuana people smoked in
dorm rooms in the 1970s,” says Staci Gruber, the director of the Marijuana
Investigations for Neuroscientific Discovery (MIND) program at
Harvard-affiliated McLean Hospital in Belmont, Massachusetts.
“You have to be careful.” Clandestine
marijuana growers have for decades been cross-breeding and selecting the
highest-potency plants to create more powerful pot.
Levels of delta-9-tetrahydrocannabinol, or
THC — the compound responsible for marijuana’s euphoric highs — in cannabis
averaged 4 percent in 1995 and rose to 17 percent by 2017, studies show.
It hasn’t stopped there. You can buy sealed
bags and rolled joints featuring marijuana strains topping 28 percent THC, and
concentrates with 85 to 90 percent.
Fortunately, plenty of products that are low
in THC and high in cannabidiol, or CBD — the other major cannabis compound —
are available.
Note: Potency varies by strain and form, and
it can often be tough to gauge a patient's tolerance.
So before a patient engages in a cannabis-based
medical treatment, he or she should consult their doctor and approach with
caution; there’s limited scientific research and, as with any medication, the
effects vary by user.
4. Edibles only seem low-risk
Hey, it’s just candy, right? But that
rainbow-hued gummy bear or little chocolate square could contain 10 milligrams
of THC, plus CBD.
That’s three to four times the amount experts
recommend for older adults.
“Edibles take from 30
minutes to four hours to take effect. It’s easy to eat more because you aren’t
feeling anything after a few minutes,” says Danielle Fixen, an assistant professor
in the University of Colorado’s pharmacy school.
“But then the effects
last six to eight hours.”
5. There’s not
enough good science about the effect on humans
And the main reason for that research gap
is that at the federal level, cannabis — medical or recreational — is an
illegal Schedule I controlled substance, legally on par with heroin, LSD and
street fentanyl.
That’s why doctors can’t technically
prescribe it; they can only give you state-required permission to use it.
More important, scientists can’t buy it at a
dispensary and study it in most labs.
That research gap means only a handful of the
common uses of cannabis are backed by substantial evidence from human clinical
trials, according to a rigorous 2017 report from the National Academies of
Sciences, Engineering and Medicine (NASEM).
Other popular uses — including for dementia,
cancer, fibromyalgia, glaucoma, depression and even insomnia — are less solid,
the NASEM experts say.
Their bottom line
(albeit two years old): “Conclusive evidence regarding the short- and
long-term health effects (harms and benefits) of cannabis use remains elusive.”
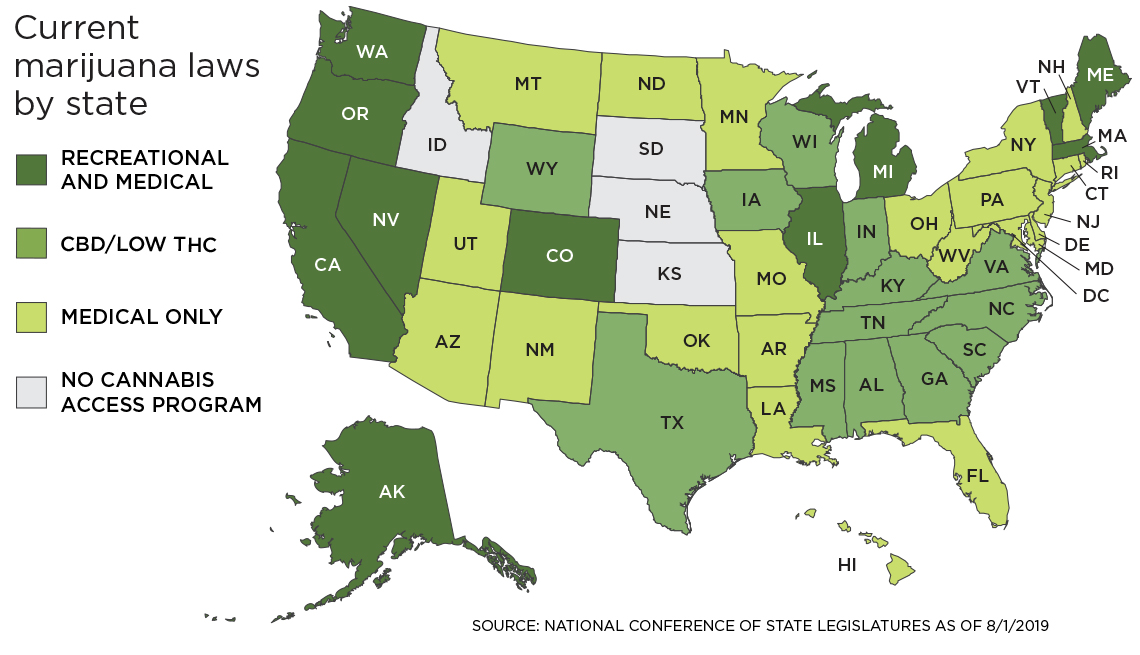 Cannabis: Where Is It Legal?
Cannabis: Where Is It Legal?
A map of the United States showing the legal
status of marijuana color coded by state
AARP
Under federal law, all cannabis is illegal to
sell, possess or use. The feds, however, are reluctant to enforce the
prohibition in the face of mounting support by states.
Thirty-three states (plus the District of
Columbia, Guam, Puerto Rico and the U.S. Virgin Islands) permit medical
marijuana for qualifying patients; a doctor’s certification and patient card
are generally required.
State laws differ on such critical questions
as who can grow it, who can sell it and what health conditions qualify. Eleven
states and the District of Columbia allow recreational marijuana use.
Under federal law, CBD (cannabidiol) derived
from marijuana, which contains the psychoactive ingredient THC, is illegal;
hemp-derived CBD that contains no more than 0.3 percent THC is legal to sell
and consume — though the U.S. Food and Drug Administration says it is illegal
to market CBD in food and supplements.
Thirteen states have passed laws allowing the
sale of CBD/low THC products.
Details vary: Check your state’s laws for the
latest info. For more information see the National Conference of State
Legislatures.
6. Marijuana’s stoner stigma persists
Whether it’s a holdover from America’s decades-long
war on drugs or pot’s still-illegal federal status, many older proponents of
medical marijuana continue to hide their use.
The lingering stigma associated with pot
keeps some people from telling their doctor, too, says Hillary Lum, a geriatrician
and associate professor at the University of Colorado School of Medicine.
“In a recent survey,
30 percent of older adults didn’t answer the question about whether or not they
used medical marijuana,” she says.
“If people feel
uncomfortable with it on an anonymous survey, they may also feel uncomfortable
telling their doctor. That could have ramifications for their health.”
7. Many doctors are in a quandary
Half of the primary care doctors working at
Mayo Clinic medical offices said in a 2019 survey that they weren’t prepared to
answer patients’ questions about medical marijuana — even though 58 percent
believed it was a legitimate medical therapy for terminal illnesses,
untreatable pain and cancer symptoms.
That hasn’t stopped some users — especially older
adults — from approaching their doctors.
“My patients want to talk about it,” Lum says.
“But I’m in an
information vacuum. We don’t have many clinical studies to show effectiveness.
Medical schools, pharmacy schools and nursing schools haven’t taught it. It’s
not in the pharmacy database we use for prescribing, so I don’t have a lot of
information about potential drug interactions and side effects.”
A few institutions have declined to embrace
its use. The Cleveland Clinic announced it would not recommend medical
marijuana to its patients when it became legal to buy in Ohio in January.
Says Paul Terpeluk, a
doctor of osteopathic medicine and medical director of the Cleveland Clinic’s
Employee Health Services, “We’re just beginning to understand the effects of
cannabinoids in the body. We do not believe states should be in the business of
regulating and promoting medications.”
But other doctors prefer not to create
obstacles to medical marijuana use.
Peter Grinspoon, a primary care physician at
Massachusetts General Hospital and a Harvard Medical School instructor, took
the unusual step of getting trained so he could certify his patients as medical
marijuana users.
“I grew up with this, so it’s hard not seeing
it as medicine,”
Grinspoon explains.
His father, the Harvard psychiatrist Lester
Grinspoon, is considered the “grandfather of medical marijuana” and
wrote a book about the history and cultural use of medical marijuana in the
1970s; there’s even a marijuana strain in Europe named after him.
His brother used marijuana while battling
leukemia, too.
“It makes sense to
try cannabis when you consider the track record of other medications a lot of
older adults take, especially for pain, sleep and anxiety,” Grinspoon says.
“Nonsteroidal
anti-inflammatories like ibuprofen and naproxen can affect your kidneys,
threaten your heart and cause gastrointestinal bleeding. Few people want to be
on opiates — they haven’t proven to work well for long-term relief, you get
constipated and they can be addictive. Sleep and anxiety drugs can leave you
sedated and may affect memory. Cannabis can be as effective as anything.”
Even nursing homes are experiencing a
profound shift toward acceptance.
One program at the Hebrew Home in Riverdale,
New York, allows residents to use cannabis capsules or cannabis oil drops and
has found that it eases pain, improves appetite and even reduced one resident’s
opioid use.
The program stays compliant with federal
rules by having residents buy and administer cannabis themselves or with the
help of a caregiver who’s not on the home’s staff.
“The benefits are
nothing short of amazing and should be more widely available to residents of
long-term care facilities,” says Daniel Reingold, the CEO of RiverSpring Health,
which operates the Hebrew Home.
The nursing home is now leading a group of
nonprofit long-term care facilities in several states planning to launch a
large study this fall of medical marijuana’s effects in older adults.
(Note: The purchase of medical marijuana from
a dispensary is not covered by the U.S. Department of Veterans Affairs,
Medicare, Medicaid or private insurance, though in some cases all may cover
FDA-approved prescription drugs, such as Marinol, that are based on cannabis.)
Where AARP Stands
In March, the AARP Board of Directors
approved a policy supporting the medical use of marijuana for older adults in
states that have legalized it.
The decision was based on the growing body of
research suggesting marijuana may be helpful in treating certain medical
conditions and symptoms.
The policy also notes that decisions related to
the use of medical marijuana should be made between a patient and a health care
provider and appropriately balance clinical evidence of benefit and harm, the
patient’s preferences and values, and any laws that may apply.
According to the
policy, “AARP also supports further clinical research of medical use of
cannabinoids to help alleviate both the symptoms of disease and the side
effects of the treatment for diseases.”
The policy adds that “AARP
believes the DEA’s [Drug Enforcement Administration] classification of
marijuana as a Schedule I controlled substance deters the medical use and
scientific study of cannabinoids” and calls on federal officials to examine
options to allow more clinical research.
Sari
Harrar
health,
medicine and science writer
I
am an award-winning freelance writer with more than 20 years of experience
covering health, medicine, and science — for national magazines, books,
custom-content publications, websites and newspapers.
Sari-Harrar-2012-400Journalism
I write for many of the most widely-read magazines and newspapers in the
U.S. My work appears in Dr. Oz’s The
Good Life magazine, Good Housekeeping, Prevention, O, The Oprah Magazine, Reader’s
Digest, The Philadelphia Inquirer, Consumer Reports on Health, Organic
Gardening and other leading publications.
Books
I’ve written and collaborated on more than 15 health-related books for major
publishers including Rodale and Reader’s Digest.
Custom
Content I produce custom content — including ghost-written books and newspaper
columns, magazine and newsletter articles and web content –for leading doctors,
major health systems, organizations, universities and corporations.
AARP is a nonprofit,
nonpartisan organization that empowers people to choose how they live as they
age.
No comments:
Post a Comment